Fascinatingly, therapists themselves vary considerably in their effectiveness
Last updated on 23rd April 2015
I wrote a post yesterday on the good, but largely stagnant, outcomes currently being achieved in psychotherapy. In today's post I highlight the fascinating finding that psychotherapists themselves vary considerably in their effectiveness. If we can help those with poorer outcomes to begin matching those with better, great gains are possible and the log jam in trying to improve psychotherapy's effectiveness can be eased. In later posts I will argue that this improvement looks eminently achievable.
(Note the ideas in this blog are explored in more detail in the chapter "Client feedback: an essential input to therapist reflection" in the forthcoming Haarhoff, B. and Thwaites, R. (2016) "Reflection in CBT: Increasing your effectiveness as a therapist, supervisor and trainer." London: SAGE Publications Ltd.)
There is considerable variation in the effectiveness of different therapists: Despite this lack of overall improvement in psychotherapy’s effectiveness over the last three or four decades, fascinatingly and very importantly there is considerable variation in therapist effectiveness. I have written about this before on a number of occasions - see, for example "Five recent research studies on the worrying variability both in psychotherapist effectiveness and also in willingness to change" and "What shall we do about the fact that there are supershrinks and pseudoshrinks?". Although the vast majority of psychotherapy studies have not been designed to detect differences in the outcomes achieved by individual therapists, there are now several research teams who have looked carefully at this area. They have routinely found that there is very significant variation between therapists. Key papers in this field include Wampold & Brown (2005) "Estimating variability in outcomes attributable to therapists: A naturalistic study of outcomes in managed care", Okiishi, Lambert et al. (2006) "An analysis of therapist treatment effects: Toward providing feedback to individual therapists on their clients' psychotherapy outcome", Lutz, Leon et al. (2007) "Therapist effects in outpatient psychotherapy: A three-level growth curve approach", Anderson, Ogles et al. (2009) "Therapist effects: Facilitative interpersonal skills as a predictor of therapist success", Kraus, Castonguay et al. (2011) "Therapist effectiveness: Implications for accountability and patient care", Saxon & Barkham (2012) "Patterns of therapist variability: Therapist effects and the contribution of patient severity and risk", Baldwin & Imel (2013) ”Therapist effects: Findings and methods”, and Green, Barkham et al. (2014) "Therapist effects and IAPT psychological wellbeing practitioners (PWPS): A multilevel modelling and mixed methods analysis".
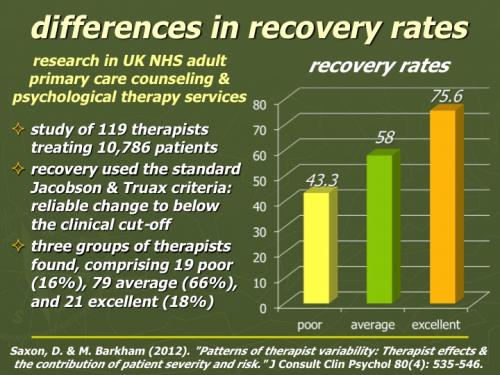
To illustrate this point, there is a recent study which looked at the therapeutic effectiveness of 119 therapists treating 10,786 clients in UK NHS adult primary care counseling & psychological therapy services. Outcomes were assessed using standard Jacobson & Truax criteria – reliable change to below the clinical cut-off. The researchers found that 19 “poor” therapists (16%) achieved only an average 43.3% recovery rate, 79 “good” therapists (66%) achieved a 58% recovery rate, while 21 “excellent” therapists (18%) achieved 75.6% recovery rates (Saxon & Barkham 2012).
(This chart is downloadable as a Powerpoint slide or as a PDF file)
And a paper published just last month (Green, Barkham et al. 2014) found that the 25% least helpful therapists in their study produced effect sizes of about 0.2, while the most helpful 25% produced effect sizes of more than 0.9 (with the most effective therapist getting considerably better results than even this impressive effect size). The authors commented "These results prompt further ... therapist effects research to sample both the characteristics and the actual 'in-session' behaviour of effective practitioners. This will then identify what it is that effective practitioners are doing differently and how this is actually clinically achieved. For example, the in-session practice of the single 'super-coach' in the present sample would be useful to sample and study." Imagine the huge improvement in service effectiveness – with major resulting reductions in suffering, disability and death – if poor therapists could learn to be as helpful for their clients as excellent therapists are.
Therapists themselves are poor at assessing their own success rates: An immediate problem with trying to implement such a potentially ground-breaking improvement strategy is that nobody really knows which therapists are excellent, which good, and which poor. It certainly seems to be a waste of time to ask therapists themselves. Remember that the Saxon & Barkham study found 18% of therapists were excellent, 66% good, and 16% poor. When mental health professionals were asked to rate their overall clinical skills and performance compared to others in their profession, 25% assessed themselves to be in the top 10%, the remaining 75% assessed themselves as above average, and none – not one – rated themselves as below average (Walfish, McAlister et al. 2012 "An investigation of self-assessment bias in mental health providers"). As Burns wrote “O wad some Power the giftie gie us to see oursels as ithers see us! It wad frae mony a blunder free us, an’ foolish notion.”